Introduction
In vitro diagnostic (IVD) medical devices play a critical role in healthcare decision-making, influencing approximately 70% of all clinical decisions. As these technologies advance and global markets expand, navigating the complex regulatory landscape has become increasingly challenging for manufacturers. The path to compliance requires strategic planning, thorough understanding of regulatory frameworks, and implementation of robust quality management systems.
Effective regulatory strategies for IVD manufacturers seek to navigate compliance pathways efficiently and successfully bring their products to market across global jurisdictions, including UK, EU and USA.
The Evolving IVD Regulatory Landscape
IVDR in Europe: A Paradigm Shift
The European Union’s In Vitro Diagnostic Regulation (IVDR 2017/746) marked a significant evolution from the previous In Vitro Diagnostic Directive (IVDD 98/79/EC). This transition brought more stringent requirements, including:
- Risk-based classification system (Classes A, B, C, and D)
- Enhanced clinical evidence requirements
- Increased post-market surveillance
- Greater involvement of Notified Bodies
- Unique Device Identification (UDI) implementation
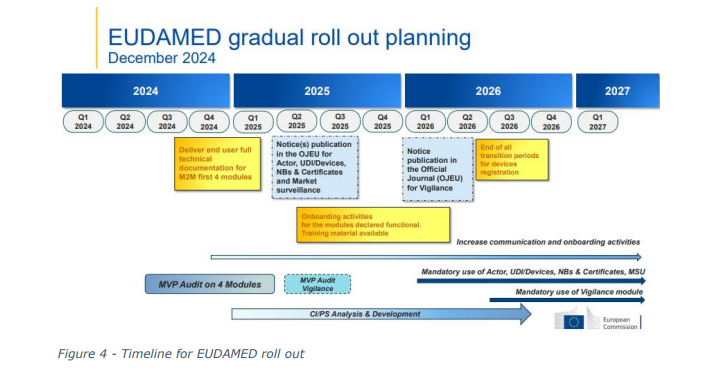
The IVDR’s phased implementation continues to present challenges for manufacturers, particularly those with legacy products requiring recertification or first-time market entrants.
FDA Approach to IVDs
In the United States, the Food and Drug Administration (FDA) regulates IVDs as medical devices, categorizing them primarily through:
- Class I: General controls (lowest risk)
- Class II: Special controls and often 510(k) premarket notification
- Class III: Premarket Approval (PMA) for highest risk devices
Global Harmonization Efforts
The International Medical Device Regulators Forum (IMDRF) continues to work toward harmonizing regulatory approaches worldwide. However, significant differences remain among jurisdictions, creating challenges for manufacturers pursuing global market access. The utilisation of IMDRF can be a valuable tool to develop a ‘one size fits all’ technical file – although this doesn’t quite work in practise. The Uks indication of using IMDRF principles is a welcome signal which may support future international recognition.
Building Strategic Compliance Pathways
1. Early Regulatory Strategy Development
Successful IVD manufacturers integrate regulatory planning into their product development lifecycle from inception. Key elements include:
- Regulatory roadmapping: Documenting intended markets, timelines, and certification requirements
- Classification determination: Early assessment of product risk classification across target jurisdictions
- Regulatory intelligence gathering: Monitoring evolving requirements and guidance documents
- Stakeholder alignment: Ensuring business, R&D, quality, and regulatory teams share understanding and objectives
Early strategic planning significantly reduces time-to-market and development costs by avoiding regulatory surprises and rework. It is important to consider the end goal – market access, and work backwards, when developing your design and development strategies.
2. Risk-Based Approach to Compliance
Implementing a risk-based approach aligns with modern regulatory frameworks and optimizes resource allocation:
- Product risk classification: Understanding how regulatory bodies will classify your device
- Risk management process: Implementing ISO 14971 principles throughout the product lifecycle
- Benefit-risk analysis: Documenting how benefits outweigh residual risks
- Risk-based quality management: Focusing QMS efforts proportionally to risk areas
This approach ensures compliance while maintaining operational efficiency. While this is a requirement to meet regulatory requirements, done right, this can add real value to the development and operational efficiency of IVD manufacturing in conjunction with ISO 13485
3. Building Robust Clinical Evidence
Enhanced clinical evidence requirements represent one of the most significant challenges in modern IVD regulation:
- Scientific validity: Establishing the analyte’s association with clinical condition
- Analytical performance: Demonstrating technical performance characteristics
- Clinical performance: Providing evidence of clinical utility and outcomes
- State-of-the-art analysis: Comparing performance against current alternatives
- Literature-based strategies: Leveraging existing scientific literature effectively
For novel IVDs, well-designed clinical performance studies with clearly defined endpoints are increasingly essential.
4. Comprehensive Quality Management Systems
A robust QMS serves as the foundation for sustainable compliance:
- ISO 13485:2016 implementation: Adopting the international standard for medical device QMS
- Process approach: Defining interconnected processes with clear ownership
- Design controls: Implementing systematic design and development procedures
- Supplier management: Controlling purchased components and services
- Post-market surveillance: Establishing vigilance and feedback systems
Integrated QMS software solutions can streamline documentation and enhance traceability across regulatory jurisdictions.
For the European Union (IVDR), Manufacturers are expected to have a compliant QMS to IVDR from June 2025.
5. Documentation and Technical File Preparation
Strategic documentation management is critical for efficient submissions:
- Common Technical Documentation (CTD): Organizing technical files in internationally recognized formats
- Modular approach: Designing core documentation adaptable to different jurisdictions
- Traceability matrices: Ensuring regulatory requirements are comprehensively addressed
- Gap analysis tools: Identifying and addressing documentation deficiencies
Electronic document management systems with regulatory intelligence capabilities can significantly enhance efficiency.
For the EU, many Notified Bodies provide guidance and template structures for how they expect to see Technical Documentation to be constructed. For classes B to D, it is recommended to engage with your NB early and understand their expectations of the conformity assessment process.
Advanced Regulatory Strategies for Complex Challenges
Companion Diagnostics
As precision medicine advances, companion diagnostics face unique challenges requiring coordinated regulatory strategies:
- Drug-diagnostic co-development: Aligning timelines with pharmaceutical partners
- Combined submissions: Navigating coordinated reviews between device and drug divisions
- Harmonized clinical studies: Designing trials that satisfy both diagnostic and therapeutic endpoints
Early engagement with regulatory authorities through pre-submission meetings is particularly valuable for companion diagnostics.
Software as a Medical Device (SaMD)
IVDs increasingly incorporate software components or exist entirely as software, requiring specialized regulatory approaches:
- SaMD framework implementation: Applying IMDRF risk categorization principles
- Cybersecurity considerations: Addressing security by design principles
- Artificial intelligence/machine learning: Navigating evolving regulatory expectations for adaptive algorithms
- Agile development: Reconciling iterative development with regulatory requirements
The FDA’s Digital Health Software Precertification Program signals evolving approaches to software regulation that may influence other jurisdictions.
Point-of-Care and Self-Testing IVDs
Decentralized testing presents unique regulatory considerations:
- Usability engineering: Demonstrating safe use by intended users
- Human factors studies: Collecting evidence in simulated use environments
- Simplified instructions: Developing clear usage guidance for lay users
- Risk mitigation: Implementing safeguards against user error
Regulatory expectations for usability have increased significantly, particularly for tests intended for self-administration.
Creating Sustainable Compliance
Regulatory Intelligence Systems
Maintaining current regulatory intelligence is essential for sustainable compliance:
- Monitoring mechanisms: Establishing systems to track regulatory changes
- Gap assessment processes: Evaluating impact on existing products and pipelines
- Strategic response planning: Developing action plans for significant regulatory shifts
- Knowledge management: Maintaining institutional regulatory expertise
Subscription services and industry associations can provide valuable regulatory intelligence resources. Examples include our partners Medboard.
Post-Market Compliance Strategies
Regulatory responsibility extends well beyond initial approval:
- Post-market surveillance planning: Designing proportionate monitoring systems
- Real-world evidence collection: Gathering data on performance in clinical settings
- Periodic safety update reports: Preparing comprehensive safety summaries
- Change management: Navigating modifications to approved devices
Proactive post-market strategies can identify issues early and support expanded indications.
Building Regulatory Partnerships
Successful manufacturers view regulatory bodies as partners rather than obstacles:
- Pre-submission consultations: Engaging early with authorities on novel technologies
- Scientific advice meetings: Seeking input on clinical evidence plans
- Regulatory inspections: Approaching audits as improvement opportunities
- Transparent communication: Maintaining open dialogue about challenges
Building positive regulatory relationships creates pathways for more efficient future submissions.
Conclusion
The evolving IVD regulatory landscape presents significant challenges but also opportunities for manufacturers who implement strategic approaches to compliance. By integrating regulatory considerations throughout the product lifecycle, adopting risk-based methodologies, generating robust clinical evidence, and maintaining adaptable quality systems, manufacturers can navigate compliance pathways more efficiently.
Success in today’s regulatory environment requires not just understanding current requirements but anticipating future developments. Organizations that view regulatory strategy as a competitive advantage rather than a necessary burden are better positioned to bring innovative diagnostic solutions to patients while maintaining compliance across global markets.
As the diagnostic landscape continues to evolve with technological advances in digital health, precision medicine, and point-of-care testing, regulatory strategies must likewise adapt. By building sustainable compliance systems and fostering positive relationships with regulatory authorities, IVD manufacturers can create pathways to market that support innovation while ensuring safety and efficacy.
How can we help?
IVDeology has a long history of working with IVD manufacturers to define their regulatory strategy based on their company goals and objectives. We establish long term partnerships with our customers to ensure they meet the regulatory requirements for market access, and through the post market phase. To learn more about how we can help, contact [email protected].